Thoracocentesis is the name given to a clinical technique whereby fluid or air is removed from the thoracic cavity.
Indications for use
* Emergency removal of air/fluid from the thoracic cavity - their presence causes dyspnoea and this must be eased to assist the animal in ventilating its lungs and hence oxygenating the blood.
* Analysis of fluid - The type of fluid removed from the thorax can be a valuable diagnostic aid:
Milky Fluid- Probably chyle, it indicates rupture of the thoracic duct within the thorax. This condition is called chylothorax.
Bloody- Blood removed from the thorax is a sign of crushing of the great vessels and is often a sequel to a crushing injury such as road traffic injury. This is called haemothorax.
If air is removed from the thorax the condition is called pneumothorax. This can be due to many things, an example of which is a penetrating wound to the thorax.
* Improved radiographs - Pleural fluid can be seen on a radiograph and is common to many diseases. Analysis of the fluid allow more accurate diagnosis to be made. Since fluid is radiodense it may obscure pathological changes within the mediastinum. Removal of the fluid will hence allow better radigraphs to be made.
This can be split into two broad categories-
Insertion of the needle
The position in which the needle is inserted depends on whether there is air or fluid present but the basic technique is the same.
* The needle is inserted into the middle of the correct intercostal space, this is done to avoid the blood vessels and nerves that run down the caudal edge of each rib.
* Aseptic conditions must be obeyed strictly and the operator should wear sterile gloves. This avoids the iatrogenic introduction of an infection into the pleural space.
* The needle is inserted at a 45' angle towards the parietal pleura preventing the lung parenchyma from obscuring the needle lumen when aspiration is being performed.
* The animal should be standing if possible but if not the animal should be in lateral or sternal recumbency.
* If the animal coughs, struggles or shows signs of discomfort during the technique the needle should be withdrawn or directed.
* Gentle negative pressure should be applied as you enter the pleural space.
* As soon as you enter the pleural space STOP and hold the needle/syringe parallel to the body wall with the tip pointing ventrally. This reduces the risk of lung laceration.
* The needle should be inserted in two steps. Firstly, the needle should be inserted through the superficial fascia, integument and muscle. Secondly, the needle should be moved dorsally or ventrally about 1cm and then inserted through the rest of the muscle and the parietal pleura. This is done so that when the needle is removed the two holes caused by the needle are not aligned reducing the risk of a pneumothorax.
* If the fluid/air is difficult to get the needle should be withdrawn slightly, before redirecting the tip. Alternatively, the other side of the thorax can be used.
* Local anaesthetic is not normally used but is useful if large volumes of fluid are to be removed.
* Since the size of the lung is reduced during expiration, if possible insert the needle when the animal is expiring.
TO REMOVE FLUID:
* In the dog thoracocentesis is performed in the ventral third of the thorax and the 6th-8th intercostal spaces. This is because the needle will go into one of the pleural recesses reducing the risk of lung laceration and will pass cranial to the costodiaphragmatic line hence entering the thorax rather than the abdomen!
* Although the position of insertion of the domestic species is not given, an appreciation of the sections on the anatomy of the pleura and lungs will allow the operator to do it safely.
* This is because as with the dog the operator should aim to insert the needle cranial to the costodiaphragmatic line, caudal to the basal border of the lung and within the ventral third of the thorax.
TO REMOVE AIR:
* This is also done in the 6th-8th intercostal spaces but at the highest point of the thorax.
* This will vary depending on the position the animal is in during the technique.
* Standing or Sternally Recumbent- Dorsal third of the thorax.
* Laterally Recumbent- Mid thorax.
Equipment required for thoracocentesis
* Sterile Needle
Cat, 18-23 gauge
Dog, 18-21 gauge
* Both of these are 1" long.
* In the larger domestic animals the gauge of the needle will increase ( to a maximum of 16 gauge) and the length will also increase to be able to penetrate the thicker muscle layers.
* Three-Way Tap- This enables multiple number of syringes to be filled without major manipulation of the needle.
* Syringe- Usually 10-30ml so that large volumes of fluid/air can be collected.
Some people prefer to use a flexible polythene catheter with removable needle once it has been inserted. This reduces the risk of lung laceration once the needle is inside if the animal was to move suddenly. It is also recommended to attach an extension tube between syringe and needle so you can manipulate the syringe without moving the needle. This too reduces the risk of lung laceration.
Anatomical structures involved Top
The most important structures involved are the lungs and the pleurae and it is essential to understand the normal positions of these. If you cannot remember, go back to the thorax tutorial and check.
Fluid is likely to accumulate in the costodiaphragmatic and costomediastinal recesses. It is therefore these places which are aspirated during thoracocentesis; this is for several reasons.
1) They present a large area in which there is no viscera, hence fluid can collect here freely.
2) Because the lung or other structures do not extend into these recesses, thoracocentesis performed here is safer since there is a low risk of lung laceration or damage to other structures.
Diagrams to show the important recesses in thoracocentesis
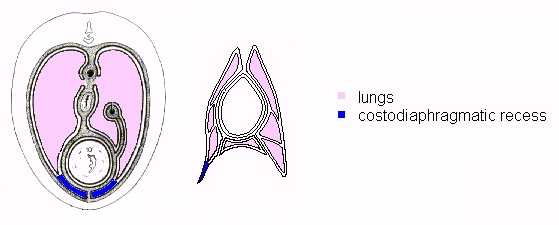
Figure 44 - Diagrams to show the important recesses in thoracocentesis
The extent of the pleural membranes
Unlike the lungs, the pleural cavities potentially occupy most of the extent of the thoracic cavity. However, as described, this space is reduced by the visceral structures.
DORSALLY
At the boundaries parietal pleura is reflected such that its two faces are directly applied to each other. Caudal to the basal border of the lung this arrangement occurs as costal pleura on the chest wall is reflected off the diaphragm forming the line of COSTOPLEURAL REFLECTION. This is important as it encloses the costodiaphragmatic recess and limits the cranial extent of the pleural cavities. The size of the recess varies with the level of section due to the convex projection of the diaphragm caudally.
CRANIALLY
Cranially the costal and mediastinal pleura dome to form CUPOLAE PLEURAE which extend past the cranial thoracic aperture.
DEVIATION OF PLEURAL CONTOUR
On the right hand side the vena cava is enveloped by a ventro dorsal extension of the pleura - THE PLICA VENAE CAVAE.
Thin pleura may allow communication between left and right sacs.
SUMMARY
Pleura are more extensive than observed from thoracic boundaries due to numerous folds. However, on the dorsal diaphragm there is a small space in which the pleura do not lie.
Comparison of the pleura in the domestic species
HORSE
The costodiaphragmatic reflection runs from the eighth rib cartilage to the vertebral end of the seventeenth rib. It slopes, is dorsocranially concave, and is projected cranially at the last rib.
The right cupola pleura extends medially.
RUMINANTS
The costodiaphragmatic reflection runs from the eighth costochondral junction to the twelfth rib, below the lateral margin of the iliocostalis. It has a steep caudal ascent and crosses the middle of the eleventh rib.
The right cupola pleura extends cranially, 2-3cm costally. Medially it regions the mediastinum.
CARNIVORES
The costodiaphragmatic reflection runs from the eighth costal cartilage to the dorsal end of the thirteenth rib. It passes the costochondral junction of the eleventh rib.
Both right and left cupolae pleurae extend, the left further than the right.
PIG
The costodiaphragmatic reflection runs from the seventh costochondral junction to the dorsal half of the last rib. It is a uniform curve.
N.B. in all species the costodiaphragmatic reflection runs from the sternum then rises at the described location e.g. eighth rib.
Clinical note:
In all species the needle must be inserted cranial to the costodiaphragmatic line or else the needle will enter the abdominal cavity.
Clinical note on the ribs:
Although the ribs are merely bypassed by the needle during thoracentesis it is necessary to know their structure for several reasons:
1) The operator should know about the prescence of intercostal spaces as it is through these that the needle is inserted. Since it is usual to insert the needle through a specific intercostal space every time the technique is performed it is useful to know the number of ribs and certain landmarks over ribs. The olecranon is over the 5th rib in large animals and the pig but over the 4th rib in small animals.
2) The presence of the caudomedial groove on the rib containing the neurovascular bundle and the needle inserted to avoid this. Hence, preferably in the middle of the intercostal space or near the cranial edge of the rib.
Remember the blood vessels!
The reasons for knowing the anatomy and hence the positions of the blood vessels and nerves which could be damaged by thoracentesis are numerous. By knowing their positions it is possible to avoid damaging them when inserting the needle and hence avoid many clinical conditions which would result from their damage. These include:
* 1) Haematoma - due to rupture of blood vessels.
* 2) Ischaemia - of muscles supplied by the intercostal blood vessels.
* 3) Neuritis - due to slight damage of the nerves.
* 4) Paralysis of the intercostal muscles- because of serious damage to the intercostal nerves which supply them. Since the external intercostal muscles are involved in inspiration, their paralysis could lead to breathing difficulty.
The muscles you should consider……
INTERCOSTAL MUSCLES
* The external intercostal - Its fibres run in a caudoventral direction, originating on one rib and inserting on the following rib. The muscle layers extent is from the upper ends of the ribs to the costochondral junctions and do not extend ventrally as far as the sternum. They assist inspiration by increasing the volume of the thorax by moving the ribcage cranially and ventrally.
* The internal intercostal - Its fibres run cranioventrally and are approximately perpendicular to the external intercostal muscles. Unlike the external intercostal muscles they do not extend to the dorsal region of the intercostal spaces, but instead they cover the ventral region around the sternum. They assist to a minor extent in expiration by pulling the the ribcage caudally and dorsally decreasing the volume of the thorax. This is only really used in forced expiration since during normal expiration the decrease in volume is primarily due to the passive recoil of the lungs.
* Transversus thoracis - This muscle originates from the dorsal aspect of the sternum. It is a triangular sheet whose apex points cranially. Slips of muscle split from the main body and run in a caudolateral direction to insert on the sternal ribs close to the costochondrial junctions. Morphologically it is the equivalent of the ventral part of the transversus abdominus. Since it is within the ribcage it lies over the internal thoracic vessels. It is involved in expiration.
You should know about the following muscles already:
* Cutaneous trunci
* Latissimus dorsi
* Pectoralis ascendens
* External abdominal oblique
* Serratus ventralis
* Serratus dorsalis
CLINICAL NOTE:
Although thoracocentesis is a fairly non-traumatic procedure, a knowledge of the muscles of the thoracic wall is necessary for several reasons.
LENGTH OF NEEDLE- An idea of the thickness of the muscle ( a consequence of the number of layers ) will decide the hypodermic needle length . If too short no fluid will be aspirated, and if too long , it risks puncture or laceration of structures more medial than the pleural space.
IATROGENIC INJURIES- (caused by the clinician) Although unlikely, if damage to the muscle occurred post-thoracentesis , it would be useful for the clinician to know which muscles were involved and so decide on therapy.